
Little did we three authors of Training for the Uphill Athlete anticipate the resulting uptick in interest in individual blood lactate testing. Since the book was published, we’ve fielded numerous inquiries from gym owners, coaches, and athletes about this testing protocol, which is especially helpful for determining Aerobic Threshold (AeT). Apparently there is a dearth of information out there, and we’re glad to have ignited some enthusiasm. This article provides a deep dive into how to conduct your own blood lactate test and analyze the results without having to go to a lab. Read on for the pros and cons of various handheld meters as well as step-by-step instructions for getting the best sample.
Before you start, be aware that there are a few hurdles to this self-exploration endeavor, from finicky devices to hard-to-master testing techniques. Buying the lactate meter is the easy part. Getting actionable information will require patience and effort.
Blood Lactate Testing for Aerobic Threshold (AeT): 2mMol/L
One of the best uses of your meter is to pinpoint your Aerobic Threshold. Nailing down this metabolic breakpoint will define the upper end of your Zone 2 and can help determine if you are aerobically deficient.
As you have read on this website and in both our books (Training for the New Alpinism and Training for the Uphill Athlete), we consider establishing an athlete’s AeT to be the cornerstone to establishing a good foundation of aerobic capacity. We encounter Aerobic Deficiency all too often in athletes lacking a good understanding of aerobic training.
There are a number of ways to find your AeT, which we explore in this article and in our books.
This current article will cover blood lactate testing in detail. We use the widely accepted blood lactate concentration of 2mMol/L to define AeT. However, some literature suggests a concentration of as high as 2.5mMol/L, and one method defines AeT as the point where lactate rises 1mMol/L above the lowest reading obtained during the warm-up or while the athlete is resting. Just be consistent with the measurement and protocol you use.
Choosing a Handheld Blood Lactate Meter
Lactate Plus
The Lactate Plus, made by Nova Biomedical, has become the most used testing device. It is reasonably priced, and the test strips are cheaper than those that pair with other monitors and it will be the focus of the rest of this article.
Lactate Plus: Pluses
- 0.7-microliter blood droplet size: You can use a very small lancet and cause less pain.
- Attractive price
- 13-second wait time from sample to reading: This speed is nice, but you need it because of…
Lactate Plus: The Big Minus
Error readings: If you use the tiny 0.7-microliter blood drop, the Plus is prone error readings. It can be really frustrating mid-test to get the big E on the screen. This is where the 13-second read time comes in handy: You can repeat the sampling without waiting a full minute. To help you limit these frustrating error readings, we have some procedural suggestions for you below.
Blood Lactate Test How To: Getting a Good Sample
This sampling process may sound identical to the operation of a blood glucose meter for diabetics—and the meter and strips look identical to those devices and strips—but the testing procedure is much trickier. Getting reliably good samples takes some practice. Don’t expect your first test be anything other than a learning experience where you waste a few strips.
Contamination of the blood sample seems to be the main reason for the Lactate Plus’s error readings. The smaller the blood sample (and the Plus can use a tiny bubble of blood), the more likely it is to be contaminated by sweat or oil on the skin. Here are some suggestions to minimize these pesky error readings.
Use a fatter-gauge lancet.
Rather than using the fine (30-gauge) lancet that typically comes with the meter, use a fatter-gauge one. You need to produce a droplet of blood sitting proud on the skin that is roughly 3 millimeters (1/8 inch) in diameter. If you don’t get that nice big droplet after about 10 seconds, do another poke adjacent to the first rather than squeezing more and harder. It is likely that you missed a bigger capillary and that the tiny hole is already clotting shut.
Do not test blood that looks thin and watery.
Your blood sample should form a viscous droplet standing up on the skin. If the sample is thin and watery looking, do not waste a test strip. It is likely to be contaminated with sweat, or the athlete is overly hydrated.
Set the depth of lancet penetration to maximum on the lancet holder.
Usually there is a scale of 1 to 5. I always dial it up to 5. You need to hit a decent-sized capillary or you will not get enough blood.
Have all your gear at the ready.
Lay out your lancet holder, meter, strips, and paper towels where you can reach them easily during the test. I like to spread these items out on a small towel. When testing outdoors, you may have to get creative by repurposing a car hood, tree stump, log, or big boulder as a table.
Brace yourself.
As the sample taker, you need something to stabilize against. The athlete is likely to be shaky, and even tiny tremors in your hands can cause you to miss the droplet or go too deep and touch the skin with the test strip.
- Finger poke: Once the blood droplet has formed, use the little finger of the hand holding the meter to steady your hand against the athlete’s hand. (If you are self-testing, you will have to do a finger poke.)
- Ear poke: Brace your forearm against the athlete’s shoulder.
If possible, do an earlobe poke.
If I’m not self-testing, I prefer to poke earlobes rather than fingers. Fingers, especially of climbers and skiers, tend to be callused, making striking a motherlode capillary nearly impossible. Plus, hands can sweat a lot, making contamination more of a problem. The skin on the ears is thin, and the lobe is highly vascularized. Just make sure to have the athlete remove any earrings.
Warm hands before a finger poke.
If it is cold out, it can be very hard to get a good sample from a finger. In cold conditions, blood flow to the extremities, especially the fingers, is reduced. To get enough blood for a good sample, pre-warm the hands fingers—either in gloves/heated mittens, with a heating pad, or by windmilling the arms vigorously until the fingers turn red. Some people suffer from a common condition called Reynaud’s Syndrome, where the finger capillaries shut down with very little provocation.
Wipe away the first drop.
Clean finger/earlobe with an alcohol swab before you poke. Squeeze out a nice 1/8-inch droplet and wipe it away with a paper towel. This also helps ensure you remove any residual oils or alcohol that could contaminate your sample.
Test the second drop—without touching the skin.
Squeeze out another 1/8-inch drop and test this one by CAREFULLY approaching the droplet with the test strip (now installed in the meter) perpendicular to the skin. If you touch the skin with the test strip on a Plus, discard that strip and start over. You WILL get an error code. When the strip touches the top of the droplet, the blood will wick up the strip and the meter will beep. This is what you want. If you go any deeper, you run the risk of touching the skin and blowing the reading.
Blood Lactate Test Protocol
When conducting a blood lactate test, the general idea is to start taking the blood samples during a 15-to-20-minute warm-up and then continue taking them at the end of each 3-to-4-minute intensity stage. If you are testing this athlete for the first time, start at what may seem like a ridiculously easy effort. Even walking is fine. You do not want to overshoot the Aerobic Threshold.
An athlete with aerobic deficiency is going to have a surprisingly (even shockingly) low AeT. By “low” I mean low heart rate, low perceived effort, and low speed/pace. Starting too fast will likely cause you to miss it. The reason for this long, gradual warm-up is that the aerobic metabolism is slow to respond to increased energy demands. In order to capture data that tells you how the aerobic metabolism is functioning, you need to make gradual changes.
The Setup
The easiest place to do this test is on a treadmill, but doing repetitive laps outdoors can work too. Whichever you choose, do the test on a gradient similar to that of your typical training and racing terrain. You may even want to do the test once on flat ground and again on steeper terrain to see if you are more aerobically efficient on flatter or steeper ground.
While you don’t need to be fasted, it’s best to avoid food within 60 minutes of the test and caffeine within 4 hours of the test and make sure you follow the same protocol each time you re-test. Take a resting lactate sample before starting the test. Elevated resting lactates (over 2–2.5mMol/L) at rest indicate increased glycolytic metabolic activity. This could be caused by that candy bar the athlete ate on the way to meet you or could indicate very poor fat metabolism. Either way, it’s nice to know resting lactate.
The Warm-up
Ensure a lengthy warm-up: 15–20 minutes of very light building to light effort (3–5 on the RPE scale). The aerobic system is slow to ramp up to meet demand and we want it firing on all 12 cylinders before starting the test. The athlete should be slightly flushed and lightly sweating, an indication that the skin capillaries are dilated. This means that the big locomotive muscles are also warmed up.
It’s a good idea to take a few samples during the warm-up, especially if the resting lactate was high. This also gives you a chance to test your sampling protocol. Normally, as the aerobic metabolism ramps up, blood lactate will begin to drop at the lower intensities of the warm-up. These warm-up samples will give you an idea of the aerobic adaptation of the athlete. If you see lactate drop from 2 at rest to 1.7, then 1.5, then 1.3, and then rise back to 1.7 again, you know that the athlete’s aerobic system is responding to the energy demands. If your athlete’s test goes from 2 at rest to 2.3 to 2.7 to 3.2 over the course of the warm-up, then you likely have an athlete who is aerobically deficient. Actual numbers will vary, but the trend of steadily rising lactates will be the same. These two scenarios are illustrated in the graphs below.
Timing the Samples
Samples should be taken no closer than 3 minutes apart, and they should be taken at the end of the intensity stage before increasing pace, heart rate, or grade. This is because the aerobic metabolic pathway takes several minutes to reach equilibrium (at these low intensities) after an increase in intensity. Ramping up the intensity too fast will leave the aerobic system playing catch-up throughout the test and will not give an accurate picture of its response to exercise intensity.
Determining the Intensity of the First Stage
During the warm-up, with the normal condition where you see a gradual drop in lactate followed gradual rise, you can determine the intensity of the first stage of the test. Here are some tips for success:
- Pick a lower starting heart rate than you might think necessary. You want to creep up on the AeT slowly from below. Overshooting will leave you wondering where it really is. Creeping up on it may cost you more strips, but you’ll get a better test (more data points). In subsequent tests, you’ll have a good idea where AeT is and you can start closer to it.
- Use a minimum of 3-minute intensity stages. Don’t worry if you go longer (4–5 minutes).
- Each new intensity stage should aim to increase heart rate by no more than 10 beats. Again, this may cost you more strips but it will keep you from overshooting. On the treadmill you can gradually increase the speed or incline to accomplish this. If you are doing the test outdoors, the athlete will need to control his or her heart rate during the stages. This intensity control is important to the collection of good data. Some athletes have a very hard time running at a consistent pace or heart rate and may need practice to dial that in first.
If you are only doing an AeT test, you can stop the test once you get readings above 3mMol/L or when the lactate reading has risen 1mMol/L above the lowest reading. For a full lactate profile, you can continue this protocol to exhaustion (see below).
Recording the Data
Collect the data by recording the peak heart rate for each intensity stage and the blood lactate concentration result for that stage. Doing this will give you enough data to plot heart rate versus lactate. Plot the lactate on the vertical axis and heart rate on the horizontal axis.
What to Do If You Get a Bad Sample
A bad sample will result in an error code or a wildly unlikely number. In either case, you will need to take another sample.
If you’ve been getting what look to be reasonable numbers like 1.7, 2.3, 2.8, etc. and then up pops a 0.3 or 13.6 at the end of the next stage, that’s highly suspect. The simplest thing to do is wait to increase the speed of the next stage until you are confident that the reading for the last stage is good. With the athlete still going along at the previous stage’s pace/heart rate, test again as soon as you can. This is where the 13-second reading of the Lactate Plus is a benefit.
Blood Lactate Testing for Anaerobic Threshold (AnT)
Lactate Threshold, Second Ventilatory Threshold, Anaerobic Threshold, Critical Power, Critical Pace, Maximum Lactate Steady State, Lactate Balance Point. It is enough to know that all these terms roughly define the endurance limit: the effort level, pace, heart rate, and power that an athlete can sustain for 20 minutes to an hour (longer for the well trained).
The normal method in these tests is to look for an inflection point where the lactate begins to rise very fast, which in theory IS the athlete’s AnT. However, there can be issues with this approach:
- It can be hard to find that inflection point in your data.
- The intensity stages are rather short so the effect you are seeing is transient.
- It can be tough to collect good samples from an athlete in this stage of near exhaustion, as they are breathing hard and can be pretty sweaty and shaky.
It would be a good idea to calibrate your findings with a DIY AnT field test (or one done on a treadmill), where the athlete essentially does a time trial at their maximum sustainable effort. The average heart rate in this test is the athlete’s maximum sustainable (endurance limit) effort. At Uphill Athlete, we use this to define the top of Zone 3. Note that less fit athletes will need to use 20- or 30-minute efforts, while very fit ones should go for 60 minutes. This is because the less fit will succumb to local muscular fatigue, causing them to prematurely slow (which will result in a lower heart rate).
Interpreting the Results of Your Blood Lactate Test
In this final section, we provide some example graphs to illustrate the range of possible results you might encounter and suggest some interpretations.
It is important to keep in mind as you review these examples that the heart rates along the x-axis will vary (sometimes greatly) between athletes. This is because people often have different maximum and resting heart rates. One person may have a resting heart rate of 40 and a maximum of 170 while their training buddy with the same performance in races might have a resting heart rate of 55 and a max of 200. The shape of the curve relative to the heart rates is what is important. After all, the reason you are doing this test is to get an individual heart rate versus lactate curve.
Sample Results: An Athlete with Aerobic Deficiency
Test #1
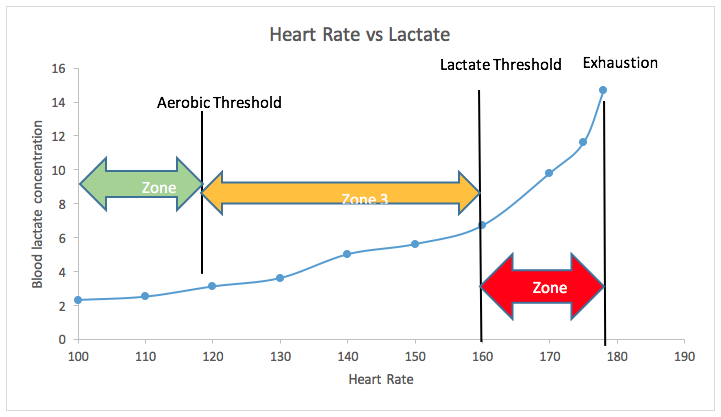
The following graph indicates that the example athlete is aerobically deficient. Notice that the lactate starts at just over 2mMol/L and climbs steadily. There is no initial dip in lactate as the aerobic system warms up. That’s because the aerobic system is not working very well and the bulk of the energy even in these lower heart rate zones is coming from glycolysis with its concomitant lactate production.
The athlete surpasses 3mMol/L at a heart rate of 118 bpm. That’s a jump of 1mMol/L, so we can set that as the Aerobic Threshold (AeT). Lactate continues to climb steadily, which is normal. Notice the slight plateauing of lactate between 140 and 150? That probably indicates that the athlete has been doing the bulk of their aerobic training at this intensity and has developed an efficiency there. The lactate curve changes pitch pretty dramatically at a heart rate of 160. We confirm this to be his Anaerobic Threshold (or Lactate Threshold) through a field test, but the inflection point on the lactate curve is also predictive of this point. We mark his AnT at 160 bpm.
Based on these results, we recommend that this athlete spend all of their aerobic training around 115–118 bpm for several months to improve their aerobic capacity and endurance.
The green arrow represents Zones 1–2. The yellow arrow represents Zone 3. The red arrow represents Zone 4.
Test #2
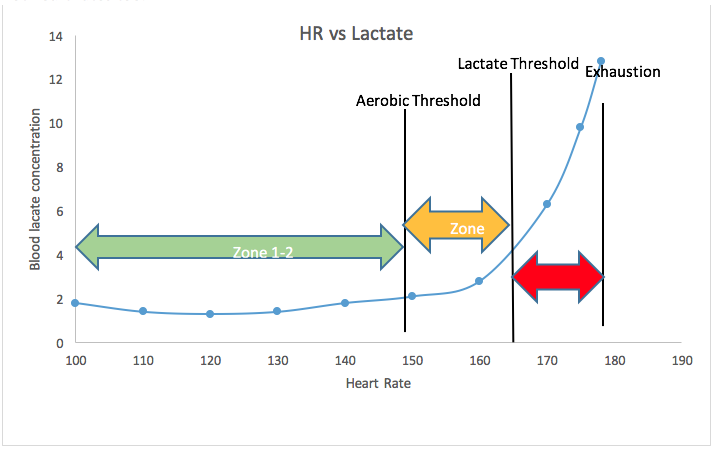
After six months of aerobic base training, the athlete returns for a retest. The results are shown below. Now we see the classic dip in lactate during the early intensity stages. This indicates that the aerobic system is using lactate for fuel at a rate faster than it is being produced. The athlete hits a lactate of 2mMol/L at a heart rate of 150—their new Aerobic Threshold. The AeT moved up by 30 beats over the six months of high-volume, low-intensity aerobic base building training.
Note the flatness of the lactate curve around 120 bpm. That probably indicates that this is where the athlete has been doing most of their training. The AnT/LT nudged up a few beats to 165—an understandably small gain given that they’ve done no intense endurance training. Zone 4 has not changed at all, again because the athlete has not done any high-intensity training.
Now that the aerobic deficiency has been corrected, the athlete can add a small volume of high-intensity training that will improve their AnT/LT. Of course, they will need to continue to do a high volume of low-intensity training to keep AeT moving up as well.
This aerobic base building can go on for years, training cycle after training cycle, with each cycle producing still higher AeT speeds if not heart rates too.
Aerobic Deficiency
In more extreme cases, you will sometimes see lactates starting well above 2mMol/L and rising steadily from there. That response is typical in athletes who have engaged in high-intensity interval training multiple times per week—think CrossFit, P90X, Orangetheory Fitness, or another popular circuit-training workout—while omitting Zone 1–2 base training. For these individuals, their blood lactate data is a graphical representation of an aerobic system that is relying almost exclusively on glycolysis for energy.
It will take months of focused attention on low-intensity aerobic work to turn this around. Figuring out what heart rate to recommend to these athletes can be near impossible. For some, a walking pace may yield heart rates of 110–120 with very high lactates. I once tested the owner of a CrossFit gym who was hitting a heart rate of 120 at a walking pace with lactates of over 10mMol/L! That may sound crazy, but that’s what happens when you focus only on the anaerobic metabolic pathway. It becomes supercharged while the aerobic path gets sidelined.
In cases like this, the first thing to do is STOP all high-intensity training and focus entirely on aerobic development—at as low a heart rate as needed to maintain for an hour or more.
You may also be interested in:
When and How to Add High-Intensity Training: The 10 Percent Test
Slow and Steady Is Boring. Is It Necessary?
Using Blood Lactate Testing in Mountain Running
1 Comment
Pingback: Applied Sports Science newsletter – November 7, 2019 | Sports.BradStenger.com