
PART ONE: The Complexity Behind the Summit — What You’re Really Training For
This past year, I coached 10 athletes directly and helped another 20 indirectly. At the time of writing this article, some are already on their way to the Everest summit, while others are departing in the next 10 days as the season winds down. It’s been a challenging and rewarding journey helping them prepare for this monumental goal.
When people ask, “How do you train for Everest?” — there is no simple answer. Although there are many answers out there, I’d like to highlight that preparing for Everest is an extremely complex and individualized process.
As a coach, my work begins with analyzing the athlete’s status. That means physical testing, physiological testing, and strength assessments. Over time, I also assess mental capacity, which is a crucial but often underestimated part of high-altitude climbing.
Next comes the climb analysis. We break down the key demands and formulate what I call the determinants of performance list. Last season, I identified about ten key factors, ranging from strength and physiology to nutrition, mental resilience, and acclimatization. Each plays a role and needs to be tested, tracked, and trained
PART TWO: The Pillars of Everest Performance, From VO₂max to Mental Grit
Once we understand the individual and the climb, we start planning the training build-up. Ideally, I have 1–2 years to prepare with an athlete. But often, I have just six months. In those cases, I quickly identify where we are and what we can realistically improve based on adaptation timelines.
We aim to improve all the key performance metrics, but often we must prioritize and focus on what we identify as the biggest performance limiters.
Key physical and physiological benchmarks include:
- Uphill speed — comparable to cycling power output, we aim for ~500 m+ gain/h or more in Zone 2 (Z2).
- Endurance metrics like VO₂max, speed at lactate threshold, and movement economy
- Durability/fatigue resistance — the ability to hold uphill speed for hours despite fatigue
- Muscular endurance — especially late-stage, for summit pushes.
- Acclimatization—ability to perform in severe hypoxia.

PART THREE: Acclimatization — Science, Strategy, and Limitations
Acclimatization is obviously one of the most important success factors and varies greatly between individuals. Some athletes perform well at altitude, while others struggle.
To assess this, it’s important to:
- Review past high-altitude experiences (e.g., Kilimanjaro, Aconcagua, other 8000m peaks)
- Conduct hypoxia tests using hypoxic generators or chambers
- Observe recovery, sleep, and physiological markers at simulated and/or real altitude
To help prepare for expedition, we apply classic and modern acclimatization strategies such as:
- Real mountain climbs prior to Everest
- Home-based pre-acclimatization using hypoxic tents or systems
- Hypoxic training methods: Live high/train low, live high/train high, combinations
The impact of hypoxia is significant because it leads to reduced recovery, poor sleep, and oxidative stress, but done right, it helps build tolerance to 6,000+ m. This can particularly support flash or fast ascents in order to climb Everest in 3-5 weeks instead of 8-9!
For more information on the huge topic of acclimatization, Listen to our podcast episode on this topic.
Hypoxic Conditioning Coaching
PART FOUR: Breathing and Recovery
Breathing mechanics and muscle strength are often overlooked, but can be critical. At extreme altitudes, lower atmospheric pressure means:
- Inhalation becomes harder
- Breathing muscles work much harder compared to sea level
We train:
- Breathing technique: Deep (diaphragmatic) vs shallow (apical)
- Breathing muscle endurance and strength
- Sleep breathing: Avoiding apneas and desaturation
Deep Breathing: Full lung expansion, with slow and controlled breaths promotes relaxation, oxygen delivery, and efficient gas exchange. Diaphragmatic Breathing (a type of deep breathing) uses the diaphragm to draw air into the lower lungs as the belly expands. This increases oxygen uptake and supports endurance, focus, and recovery.
Shallow Breathing: At altitude, often by default we turn to subconscious, quick, and minimal chest movement (upper lungs only). During apical breathing we use the upper chest and neck muscles (apex of the lungs) to breathe. This is a less efficient way of breathing that is common under stress or a result of poor posture and can lead to fatigue or anxiety.
Breathwork techniques can help reduce sleep apnea at altitude, especially the central type caused by unstable breathing during sleep. At high elevations, low oxygen often leads to over-breathing, which lowers carbon dioxide (CO₂) levels too much and causes the brain to pause breathing during sleep. Breathwork—such as slow nasal breathing, diaphragmatic breathing, and breath-hold training—can improve breathing control, increase CO₂ tolerance, and support more stable nighttime respiration. While not a replacement for medication in severe cases, regular breathwork can be a useful tool to support better sleep and acclimatization in higher altitude environments.
There are also breath-hold and CO₂-tolerance techniques that might offer small benefits. But the goals are clear:
- Improve oxygen uptake
- Delay desaturation
- Reduce physiological stress
All of this can enhance sleep, recovery, and function above 6,000 m.
PART FIVE: Monitoring Progress and Staying Healthy on the Mountain
Finally, we integrate all components into a performance-readiness model in TrainingPeaks to monitor training load and account for additional stress from other factors.
Chronic training load (CTL) in TrainingPeaks helps us to monitor fitness, fatigue and adaptation to training.
We also incorporate subjective feedback, lab and field testing, and hypoxic performance profiling to ensure an optimized training response—avoiding both overreaching and undertraining.
Health management is crucial. Infections, poor sleep, or overtraining can derail the progress, so it’s important to teach athletes to monitor early signs of:
- Altitude illness
- Poor adaptation
- Recovery (monitoring RHR, HRV, SatO2)
We also train the gut and hydration strategies needed to perform at altitude. Knowing what to eat, drink, and supplement with above 6,000 m is a huge part of the game.
Ultimately, success on Everest is about minimizing impact of severe hypoxia, maximizing readiness, and understanding the interplay between physiology, psychology, and extreme altitude.
I’ll keep refining this process. But what I know for sure: there is no shortcut. It takes methodical planning, time, and deep respect for the mountain.

PART SIX: Mental Resilience and Strategy
Hearing my athletes’ stories—when they have been spending weeks and possibly months on the mountain—has made it clear just how intense the process is. It’s an amazing journey, of course, but also one filled with uncertainty, discomfort, and adversity. There’s a lot of time on your hands when you’re up there. That means time to think, overthink, and sometimes spiral into anxiety or doubt. Most of the athletes I coach have had to deal with some form of infection—it’s incredibly hard to avoid that at altitude.
The ability to deal with adversity becomes absolutely critical. Not just because of the physical hardships like cold, pain, low oxygen, but because of the mental load. Being able to actually show up on summit day, mentally focused and emotionally grounded, without having drained all your energy by worrying or burning through your mental reserves, is key. Mental fatigue can be just as damaging as physical fatigue.
That’s why mental training has to be part of the Everest preparation plan. As we’ve seen in other endurance sports, from ultra running to triathlon, athletes rely on specific psychological strategies to get through extreme fatigue and discomfort. Developing coping tools, practicing visualization skills, and emotional awareness helps athletes face the unknowns and push through barriers.
PART SEVEN: Strategy & Pacing on the Mountain
As a coach, my influence on how the climb is organized is limited., but I try to make sure my athletes go with solid companies that have reliable plans, especially around rotations and summit pushes. The challenge is that these climbs are not always predictable. Weather shifts, conditions deteriorate, and suddenly your summit window opens earlier than expected. That means going when you’re possibly not fully recovered, after a bad night’s sleep, or in a compromised state. Sometimes, pacing goes out the window because of crowding on the route.
Rotations up to the higher camps are tough and very draining, especially when rest and recovery back at base camp is limited. Everest BC is at 5400m, which is very high and will affect your body negatively after several weeks. The entire process taxes both body and mind.
I’m aiming to create a better monitoring system to support my athletes through these unpredictable, high-stress scenarios. I want to make sure they are as ready as possible—physically and mentally—for the wide range of demands they’ll face.
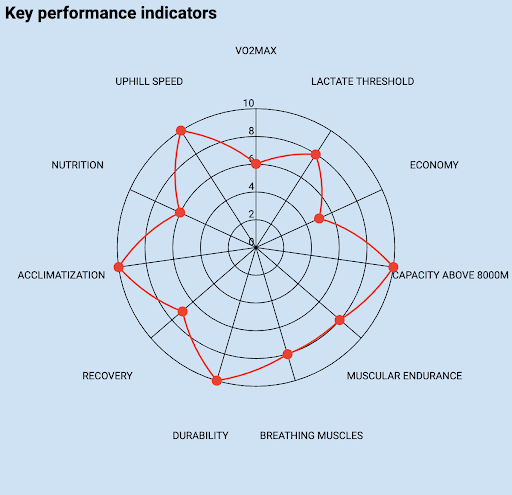
PART EIGHT: What does it take to climb Everest?
Your physical capacity must be at its peak. The earlier you begin your preparation, the better, because meaningful adaptations take time—weeks, months, even years. There is no single number or metric that can tell you if you’re “ready.” It’s not that simple.
Instead, we use a list of key performance indicators (KPIs) that group the various capacities needed to succeed: endurance, uphill speed, fatigue resistance, strength, recovery, nutrition, acclimatization, breathing capacity, and mental resilience. We test and train these systematically.
This gives us a realistic, actionable plan that maximizes your chances of success.
Start early. Be patient. Build each training block. The better you understand your own strengths and limiters, the more you’ll understand about your ‘WHY’ in training.
Everest is possible, but it demands your best. As a coach, my job is to make sure you’re ready, not just to climb, but to endure, adapt, and ultimately succeed.
Sometimes, despite your best effort, the summit doesn’t happen. I want to mention this, because we mostly hear the success stories. But as an athlete, I’ve often come home “empty-handed.”
Still, I never defined success solely by standing on a summit. The real achievement is showing up and giving it everything I have. Everest is the highest mountain on Earth — it demands respect, patience, and humility.
In races, there’s only one winner. Are all the others losers? Of course not. Turning around and going home safely isn’t failure. Sometimes, it’s the bravest and wisest decision you can make.
Suggested Additional Reading:
Understanding Altitude: An Overview for Mountain Athletes
Training for Everest: A Coach’s Perspective
Table of Contents