The problem is uncertainty
Every endurance athlete who trains with a heart rate monitor has had the same experience. You step out the door for an easy aerobic run, settle into what you believe is the right effort, and finish the workout unsure whether the physiological work you did matched what you intended to train. You had a number you were following, yet you do not actually know if the number was right.
The aerobic threshold (AeT) marks the point where your body’s reliance on fat as a primary fuel source begins to give way to carbohydrates. Your aerobic and glycolytic energy pathways are always working in concert; there is no switch that flips from one to the other. What changes with intensity is the balance. Below AeT, fat oxidation dominates, lactate production and clearance remain in equilibrium, and the adaptations that make endurance possible are built most effectively. Training above AeT, that balance shifts and carbohydrate becomes the dominant fuel, lactate production begins to outpace clearance, and fatigue accumulates more quickly. The workout that was intended to build fat oxidation and aerobic endurance has quietly become something else: a harder effort pulling toward anaerobic metabolism, with a different stimulus and a different recovery cost.
The problem is not effort. It is uncertainty. Athletes who care about the work do the work. What they cannot do, on their own, is know whether their effort during the workout matched the intent of their training. Until now.
This is the gap Continuous AeT is built to close.
What Continuous AeT does
Continuous AeT is a feature inside the Uphill Athlete Training Groups dashboard that reads an athlete’s training data each week and proposes an updated aerobic threshold based on what their data reveals. It looks at the relationship between heart rate and pace or power across sustained efforts, watches for drift patterns in those efforts, and produces an estimate that the athlete can then accept or reject.
Continuous AeT brings the kind of pattern recognition that comes from reading thousands of training files directly into the athlete’s own dashboard, if the reading is accurate enough to trust.
Why we tested our own work
Before we offered Continuous AeT to any athlete as a real input to their training, I wanted to know how it compared against the way I would score the same athletes sitting with their data myself.
This is not the only useful reference point. Lab testing, ventilatory threshold work, and well-executed field tests all give high-quality AeT values. But field-trained, file-by-file coach judgment is the closest reference we have to the question the athlete is actually asking, which is: what effort level should I be training at on Tuesday morning, and is my current HR estimate close enough to trust?
So we tested Continuous AeT against that reference, in the most honest way I could design.
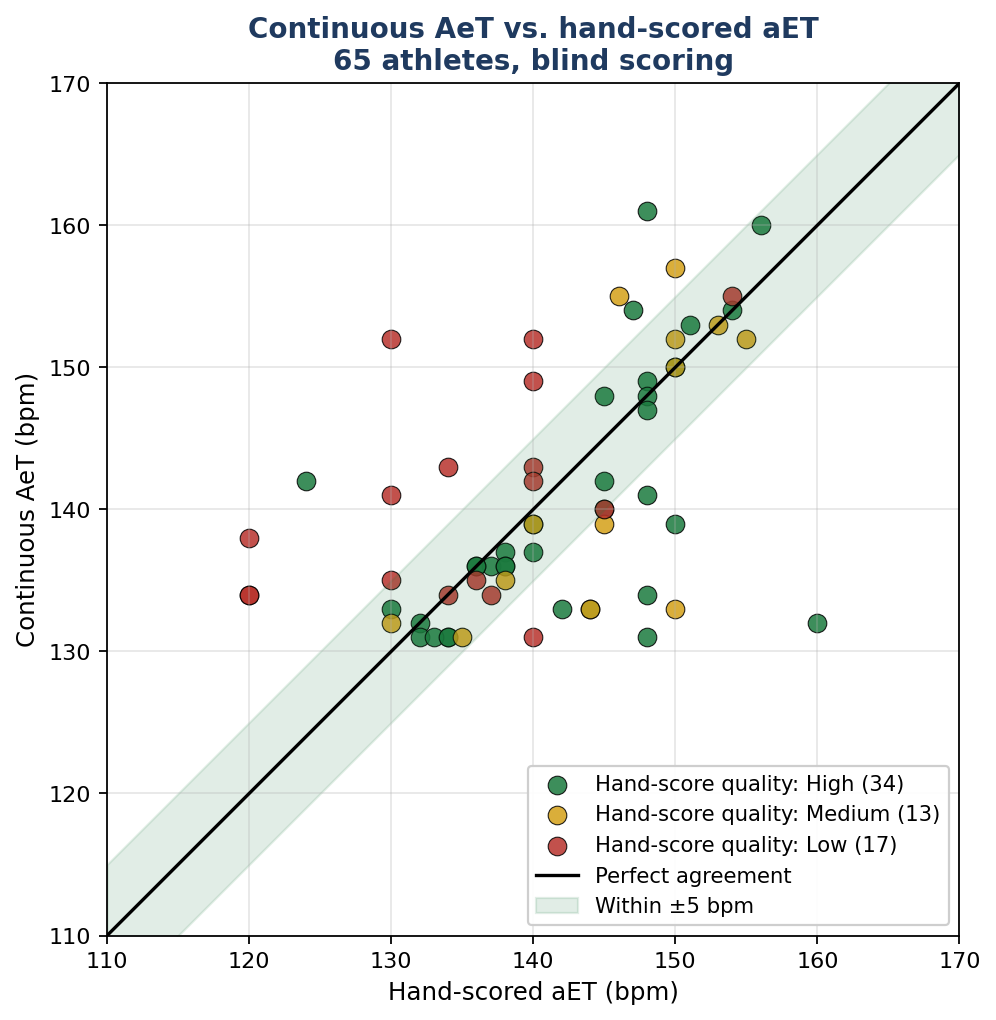
How the test was run
We pulled the training files of 128 Training Groups athletes and ran Continuous AeT against each one. I then sat with each file and hand-scored an AeT for the same athlete, working from the same training data the tool used, without seeing the tool’s Continuous AeT value. For each athlete I also recorded my confidence in my own score, on a three-level scale of clean data, mixed data, and sparse or messy data. The data we used was real. The scoring was blind on my side.
Of the 128 athletes, I produced a confident hand-scored AeT on 65 of them. On another five, the data was too sparse for me to score honestly, and I marked them as such. The remaining athletes had not yet been pulled into the manual scoring queue at the time of this analysis. Hand-scoring takes hours and 65 paired observations provided enough data to form a statistically meaningful agreement test.
What we found, in plain language
Continuous AeT is unbiased on average
Across the 65 athletes I hand-scored, the average difference between Continuous AeT and my reading was 0.1 beats per minute. The tool is not systematically too high or too low when you look at the whole group.
Continuous AeT outperforms what athletes set for themselves
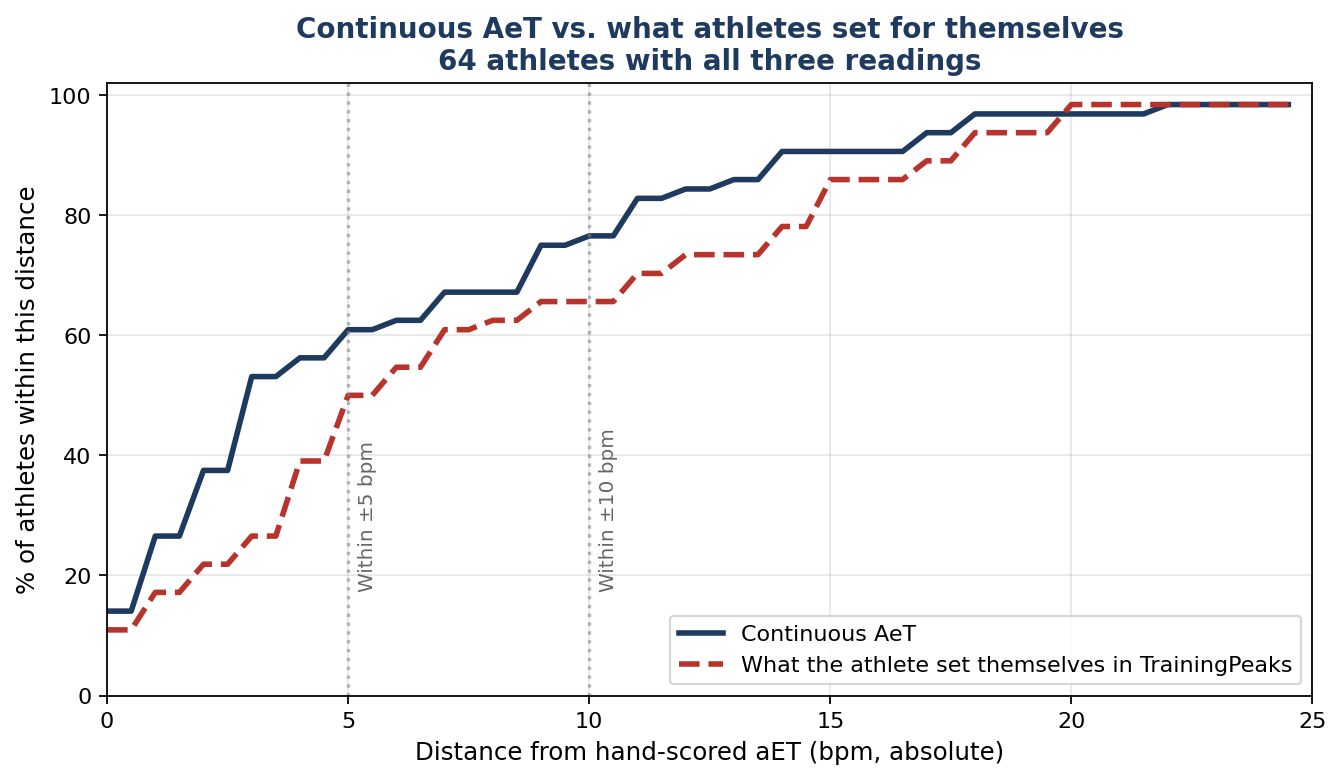
Most athletes in our Training Groups have set their own AeT using our Aerobic Threshold Test. Continuous AeT was significantly closer to my hand-scored value than the athlete’s own settings. Athletes, on average, set their own AeT about 4 beats per minute too high. Continuous AeT does not do that.
This matters because the realistic alternative to Continuous AeT, for most athletes, is the value the athlete picked themselves. In that comparison, Continuous AeT is clearly the better starting point.
The average hides the most interesting finding
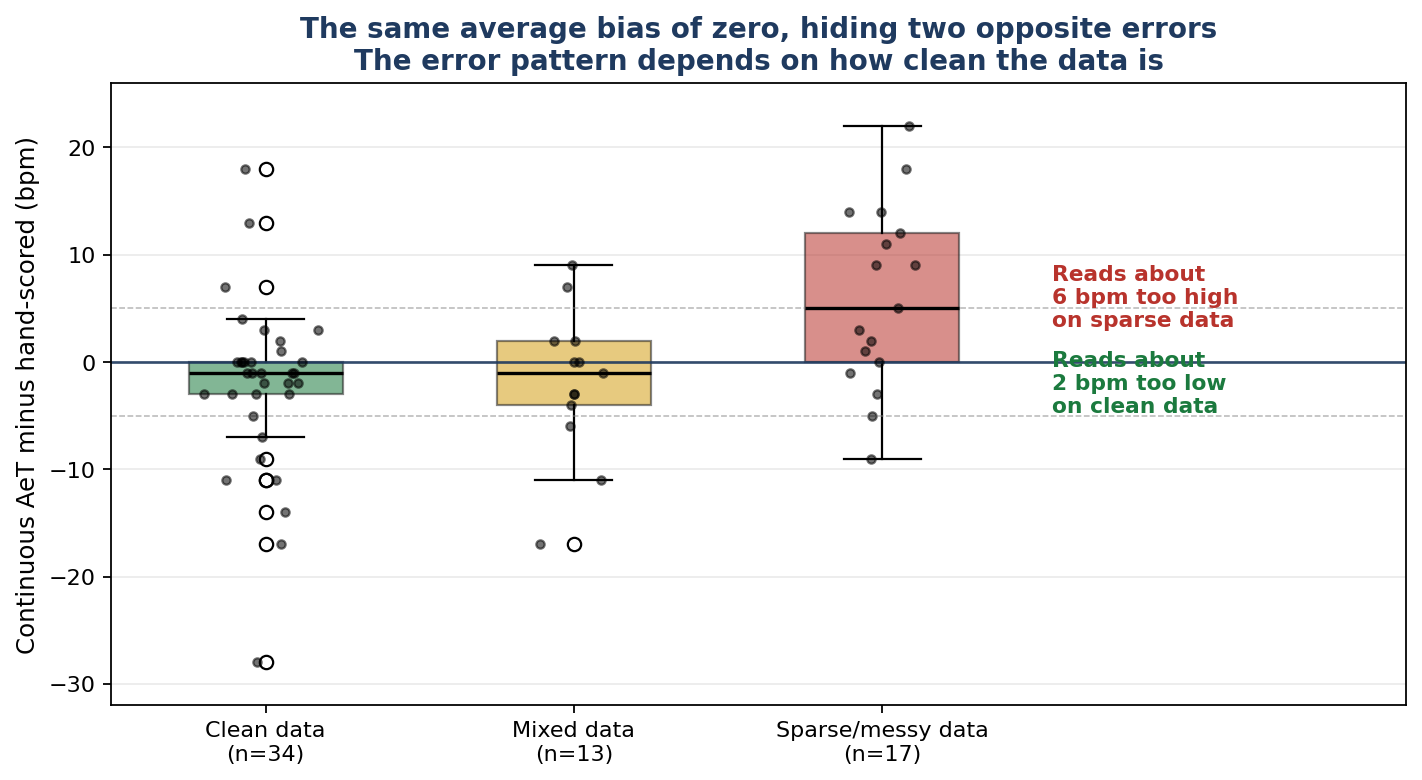
When we split the 65 athletes by how clean their training data was, the centered average pulled apart into two distinct patterns.
For the 34 athletes whose data was clean enough for me to score with high confidence, Continuous AeT read about 2 beats per minute lower than my value. For the 17 athletes whose data was sparse, inconsistent, or otherwise noisy, Continuous AeT read about 6 beats per minute higher than my value. The 13 mixed-data athletes sat between the two.
On average the errors cancel out, but averages describe groups, not individuals. For any individual athlete, the direction of the error matters a great deal. The athlete with clean data sees a number that is slightly conservative, which is the safer direction. The athlete with sparse data sees a number that is too high, which is the more harmful direction, because an AeT set too high pushes easy training into intensities that compromise aerobic adaptation.
This was perhaps one of the most interesting findings in this process and it really has shaped how we are choosing to roll the feature out.
The range of disagreement on any single athlete is wide
Roughly 62 percent of athletes saw a Continuous AeT reading within 5 beats per minute of my hand-scored value, and roughly 77 percent were within 10 beats per minute. The 95 percent limits of agreement, which describe the range within which most paired differences fall, sit between 17 beats below and 17 beats above zero. The center of the distribution is reliable. The tails are wide enough to be taken seriously.
What we are doing about it
Three decisions follow from what the analysis showed us.
We are launching Continuous AeT inside Training Groups first
The Training Groups environment was built for the athlete to be the governor of their own training. Our new dashboard lets the athlete see the proposed AeT, see the training data behind it, and decide whether to apply it. Nothing changes in the athlete’s training zones without that explicit confirmation.
For athletes who work 1:1 with an Uphill Athlete coach, training zones will continue to be manually set and evaluated by their coach. A coach has the full context and a deep understanding of the athlete that a formula can never replicate.
We have built in a refusal layer, not just a calibration layer
The clearest signal in the analysis is that the dangerous failure mode happens on athletes whose training data is sparse, inconsistent, or noisy. The right response is to refuse to run the Continuous AeT tool on this data. This refusal layer is built into the Training Groups release. Athletes whose data is too sparse to read honestly will see a tile telling them that their training file does not yet have enough signal for a confident reading, and the proposal will be withheld for the next weekly pass. Five athletes in the test set fell into this category, and the fact that they were easy to identify was one of the more useful things the test showed us.
We are publishing what we found, including the parts that are not flattering
This part is a choice about who we want to be. The training industry is full of products that ship first and explain themselves later, if ever. Uphill Athlete has been built on education and transparency about the underlying processes. Athletes who use Uphill Athlete tools deserve to know how those tools were tested, what they do well, and where they have known limitations.
If a careful coach would not score the file by eye, the tool should not score the file either.
What this means for athletes training with us
If you are in a Training Group, you already see Continuous AeT proposals in your dashboard.
If your training data is light or interrupted, you may see no proposal for a stretch of weeks. That is the refusal layer doing its job. It will soon be able to explain what is missing in order to generate an AeT reading reading that we can all trust.
If you work with an Uphill Athlete coach, Continuous AeT is not currently part of that workflow. Coach-reviewed threshold values carry context and judgment that the tool cannot replicate, and we are being deliberate about how and when Continuous AeT fits into that process. Hand calculated values are still the gold standard and your coach remains your best resource for threshold updates.
If you train on your own, outside of Training Groups, and you want to bring more certainty to your AeT, two paths are open. You can join a Training Group and have your AeT tracked weekly. You can start working 1:1 with an Uphill Athlete coach, where AeT is one of many anchors a coach holds for you. Either path replaces guessing with structure.
Methodology and acknowledgements
The agreement analysis used 65 paired observations, drawn from a Training Groups data pull on May 21, 2026. Hand scoring was done blind to the Continuous AeT value. Agreement was assessed using mean signed difference with a 95 percent confidence interval, mean absolute error, root mean squared error, and a Bland-Altman framing with 95 percent limits of agreement. Tolerance bands were set at 5 beats per minute and 10 beats per minute, chosen because they correspond to less than half and approximately a full training zone range, respectively, at the heart rates that anchor AeT for our population.
Subgroups were defined by the data-quality confidence I recorded during hand scoring, by fitness as measured by Chronic Training Load, and by 14-day plan compliance. The Wilcoxon signed-rank test was used to assess whether the subgroup biases differed from zero. The sparse-data subgroup bias of approximately 6 beats per minute is statistically significant at the conventional threshold. The clean-data subgroup bias of approximately 2 beats per minute is borderline. The 95 percent confidence interval on the overall bias is 2.1 beats per minute in each direction.
The remaining 63 athletes in the data pull have not yet been hand-scored. The next step in the validation work is to prioritize sampling from the sparse-data subgroup, where the tool is most likely to produce an inaccurate reading, rather than scoring all 63 sequentially.